Ask yourself two simple questions this week:
“What if all the COVID case data we based government policy on was inaccurate?”
“What if every single scary statistic is based on a COVID test which is being misused?”
We believe we are about to see the entire ‘casedemic’ decision making framework dismantle as the PCR testing debate gets put to more mass debate and scrutiny. Why? Thanks to no other than Elon Musk. A man that has 40 million followers on Twitter. This week he tested positive (twice) and negative (twice) off the same machine, posted such on his twitter account and the twittersphere has gone to a new level of scrutiny.
How this debate unfolds is going to be an important driver of the next leg of our Lockdown Stock Series (more in the next post….).
Key Takeaway?
The takeaway is that we are doing mass testing of asymptomatic people (or people with related seasonal symptoms) at such high testing sensitivity that we are just picking up tiny fragment and debris of the COVID virus. As a result, a lot of cases are not at a stage where the person has symptoms or is even contagious. Is this possible and could we be seeing the greatest statistical mistake in modern history?
How is this level of error possible? What is a PCR test?
Lets try and keep this simple but its important to understand the debate (and we believe this will not even be a debate shortly).
- There are 4 things we need to create living organisms – lipids, proteins, carbohydrates and nucleic acids. Within nucleic acids there are 2 groups RNA (single strand) and DNA (double strand). A virus uses RNA to capture its genetic information.
- A PCR test is used to identify RNA sequences that are unique to SARS-CoV-2 and this is what is used to arrive at the vast majority of case numbers we see everyday. This is different to antigen and antibody testing which you can read more about at the bottom links.
- How does a PCR test work? It is very technical, but here are the basics. It was invented in 1980’s and is fundamental to much of genetic testing. The genetic sequences captured through a swab i.e your DNA/RNA, is amplified up to allow for the testing.
- What is this amplification? This is really important to understand and we believe is going to be the focus of much debate. The PCR uses thermal cycling (heating and cooling) to break down the sequence to allow us to test for RNA.
- How many cycles are used is becoming the ‘hot topic’. Typically a PCR consists of 20 to 40 cycles. The number of cycles used is becoming a major focus. As you go through each amplification or cycle threshold you run the risk of saying smaller and smaller amounts of RNA from the original sample are present – even though there is so little virus (viral load) that the person has no symptoms nor is contagious.
- Now this is the amazing bit – the cycle threshold is typically not included in the results provided back to the patient or doctors. It is just a binary positive or negative.
- How wrong could we be? In August 2020 , the New York Times did a study on 3 sets of positive COVID testing data and found that 90% of them contained very little virus. This is a factor everywhere. In October 2020, the clinical advisor to the HSE (Ireland’s Health body), Dr Colm Henry, said that 80% of the cases in Ireland were mild or asymptomatic.
- When is a Case a Case? This is important – a probable case in most countries is someone that presents themselves to a doctor with symptoms. A confirmed case is a PCR test. In the UK, there has been an explosion in Pillar 2 PCR tests (this is done at home/drive through) but you never see a Doctor. So now a doctor hasn’t see you and you are prone to a highly sensitive test prone to error. We are now exposing the flaws in a PCR test.
- But wait….can’t someone with no symptoms spread the virus? This is where it gets interesting. Studies have found that after 3 to 4 weeks the presence of virus in hospitalized patients is effectively gone and the person is no longer infectious. To show infectious, someone testing positive on a PCR (possibly a fragment of RNA) you then have to take the virus and inject it into a cell culture to see if it can reproduce – something that is not being done. Scientists, including the US top official, say that if you cycle 35 times to find the virus the likelihood the virus could replicate i.e infect others is almost non existent.
- But surely the government would not make this great a mistake? The answer is yes. Let us listen very carefully to what the US government is saying. Dr Fauci said in a July interview that if you get a cycle threshold of more than 35 the likelihood of the virus being contagious is negligible.
- The University of the Oxford has found fragment of the virus 10 weeks later when you run to a very high cycle threshold i.e amplification.
What’s the conclusion? Cycle threshold above 35 is nonsense.
The tests are unreliable. The PCR test forms the basis of almost every case, hospitalization and death statistic you have seen. This is a highly infectious virus that was much more widespread but now we are picking up fragments of virus, in labs and drive throughs, with anyone with a cough or a temperature that no longer has COVID.
What cycle thresholds are governments using?
The number that keeps coming up is the risks of false positives when you use a cycle threshold above 35. Actually, the right number for someone to be infectious is probably 25.
At a government hearing in September 2020, Professor Carl Heneghan stated that NHS guidelines allow for cycles up to 45. Simply amazing. We saw a comment that the WHO guidelines are 50 but have not been able to find a document to verify that.
Every citizen should ask the government for release of information on how cases were calculated and under what cycle thresholds. SAGE in the UK, and their equivalent in every country, should be open to peer review and scrutiny.
What about hospitalizations and deaths?
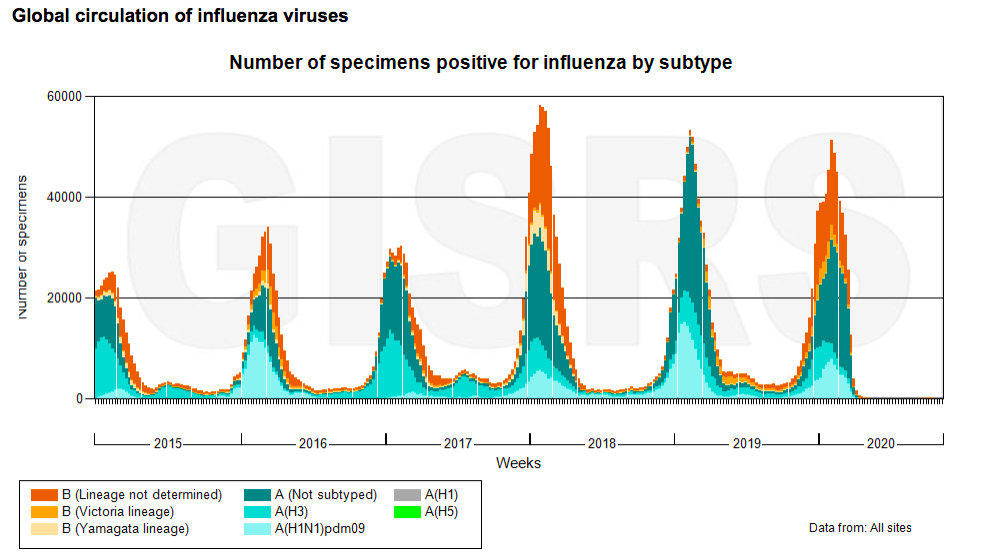
2 simple points. Is this person in hospital suffering from other diseases? As the chart below shows – flu has miraculously disappeared. We also know that deaths, once captured with a PCR test, show a very high level of co-morbidity with people with other symptoms and an average age that is in line with normal periods. Also, excess deaths have disappeared.
What should the Government do?
First step, will be the inaccuracy of the test is about to be called out. The threshold for calling a case a case will change and someone being labelled infectious will shift.
This means the entire lockdown framework is about to be called into scrutiny as the core of whether you can travel, go to a restaurant or to work is based on false cases. This is not the dangerous , spreading disease as being described to the public. Lockdowns will end.
The high risk groups will have the Pfizer vaccine available to them from next month in the UK. People will have assurance that the higher risk groups are getting protected. The Astrazeneca and University of Oxford results are speculated to be positive and they need to be distributed at 2 to 8 degrees which is in keeping with refrigerated food logistics versus the minus 70 degrees for Pfizer.
Was the entire western world misled? Is that possible?
In 2021, Morgan Stanley estimate that Pfizer and BioNTech will make $14bn of revenue from their vaccine. As Charles Munger (Buffet’s right hand man) said “Show me the incentive and I will show you the outcome”. I will let you read the outcome of the European hearings in 2010 (link below) into Swine Flu and scaremongering by WHO and the European Health Authorities at the time – findings show that they were heavily influenced by the pharmaceutical industry at the time and it brought bias to their research. Did governments have perfect information in March/April – no. Do they have perfect information now? I have never seen so much analysis.
What for our Lockdown Series? Separate post to follow.
We will provide a full post in due course but needless to say we expected a shift in sentiment, it has happened and we highlighted industry leaders with 100% to 200% upside on a 2 year view. Some of the recommendations are up 20% or 30% since writing. No change of view until they have reverted to their typical revenue, profits and normal valuation multiples. $GME , $MAB.L, $HSW.L, $HEAD.L
Finally, flu has disappeared. Riddle me that…..
We haven’t digged too deeply but it looks like seasonal flu has disappeared? Maybe they are all getting tested for Covid….
Reference articles
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa619/5841456
https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
https://www.cebm.net/covid-19/pcr-positives-what-do-they-mean/
https://assembly.coe.int/CommitteeDocs/2010/20100604_H1n1pandemic_E.pdf
Collective Finance Research
The GameStop Short Squeeze is coming
Lot’s more to follow….
The Collective are a panel of stock enthusiasts writing about high conviction investment opportunities with high return potential.
Visit our website for more.