The purpose of the Collective is to focus on mispriced securities. Our core view, in the “Post lockdown” series, is to look out to 2021 and 2022 and to not try and time the COVID dynamic week to week nor try and be a medical expert. Saying that, when we start to see medical professionals question the framework that governments are applying to the COVID crisis we do pay attention and have spent time reviewing some academic and opinion pieces this weekend.
All over Europe and the US now we have elaborate warning systems and protocols reacting to ‘cases’. A constant feature of the COVID crisis has been the narrative and definition, or lack of, around statistics. A reminder of the challenges that have been discussed year to date:
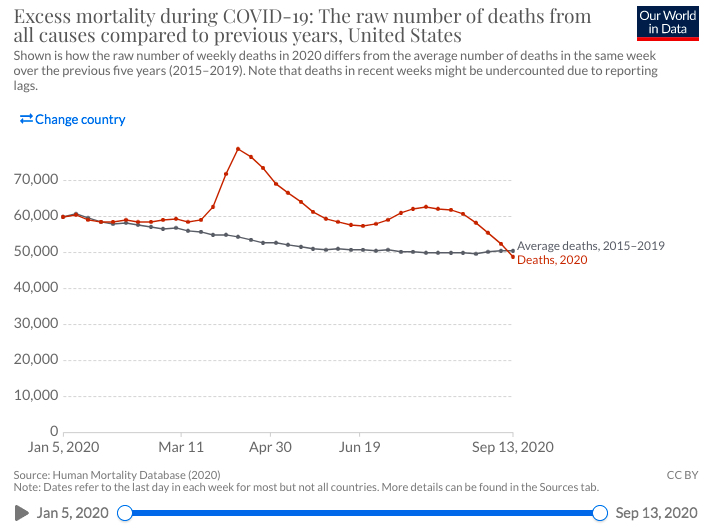
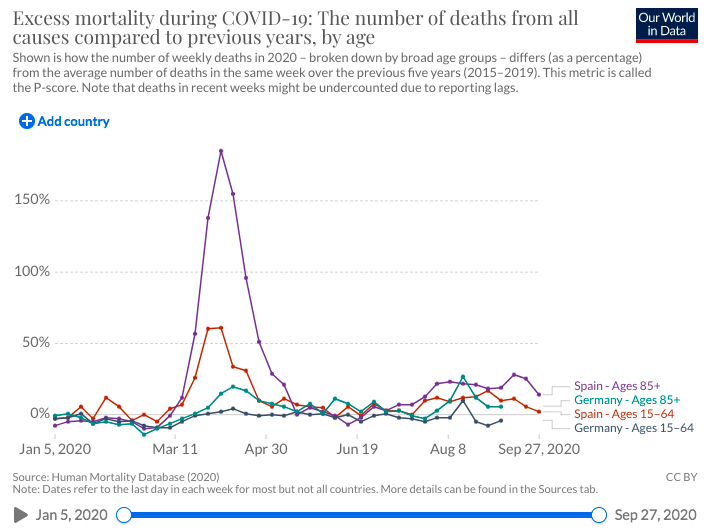
- Mortality – every country has taken a different approach to capturing whether someone died “from or with” COVID. In most countries, the median age of deaths is in the 80’s and 90% of people have other conditions. This is normal average age of death compared to pre COVID periods. To see where we are in this crisis, and given the challenges of definition, a lot of common sense analysis has stated that the only approach is to look at excess deaths i.e how many people more versus historical average have died in the current period (regardless of the reason for death). Separate to the flaws of measurement, the WHO warnings of the number of fatalities expected from COVID in March and April could not not have been more wrong. Thankfully, in every country excess deaths have declined to normal levels. See Chart 1 and Chart 2 for excess death normalisation.
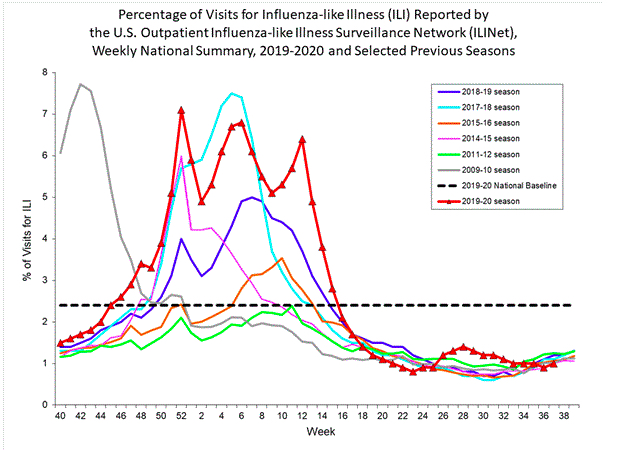
- Hospitalisations – we will misinterpret rising hospitalisations in coming weeks and the government and the media will be to blame. In coming weeks, as is normal with flu season, we will see more people present at hospitals with flu systems. Many of these will be tested for COVID, using a PCR test and all the flaws associated with such, and we will say these are COVID hospitalisations. The policy makers will react and discuss ICU and hospitalization risks, but the question we will not ask will be “how many people present themselves with flu like systems in a normal year?” See Chart 3 for the dynamic in the US – it would appear hospital visits for influenza like symptoms are now behaving like normal (albeit it with a lag as data is collected). To complicate matters, occupancy in hospitals in the summer was very low and many procedures for other conditions were deferred due to fear we created. https://www.bbc.com/news/health-54440392
- Cases – this is the statistic that has received the most scrutiny by the medical community in recent weeks. We all bought into the WHO doctrine of “Test, Test, Test” which has become “Case, Case, Case”. We are using a RT-PCR test to capture cases in the western world. There are some significant flaws with this approach. In the UK there has been a ramp in what is called Pillar 2 testing (this is away from hospital and in a commercial lab or a drive through using a PCR test). There are some serious questions over the flaws in this approach which medical researchers are starting to highlight. We will discuss that below.
Flaws in PCR testing for COVID
Firstly, evidence of a virus by a PCR test does not mean a large viral load of sufficient measure that you are ill or are going to become ill. This has been at the core of the growing number of questions being asked of the government obsession with cases under PCR test. There are fragments of this virus everywhere and we are testing people that do not have symptoms. This recent article in the Lancet Journal articulates the issue:
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30453-7/fulltext
In summary, in the UK in April and May people that were tested were severely ill and in hospital. We went from 3,000 hospital admissions per day in the first wave to about 100 per day in August. However, the number of UK tests went from 12,000 per day on 1st April to 200,000 per day on 1st August. So we went from testing people with severe conditions in hospital in April to testing large groups of people with no conditions in August and September. So what has happened next? Yes, more cases and the casedemic.
“Test, Test, Test” becomes “Case, Case, Case” but what do cases actually mean?
A growing number of questions about the framework we apply has been building through the month of September. Firstly, there was an open letter (https://docs4opendebate.be/en/open-letter/ ) from a group of Belgian doctors in early September to the government and public questioning their approach and claiming their focus on restrictions and cases was causing more harm than good.
A number of weeks later we have seen doctors in Ireland question the lack of balance and singular approach to COVID cases, without considering the declining risks, at the expense of the broader well being of society. They also called out the flaws in using a ‘swab’ without further diagnosis to identify cases. Those doctors have been dismissed from their posts (Dr Martin Feeley and Dr Patrick Morrisey). The deputy Prime Minister in Ireland (a doctor by training) publicly opposed the recommendation from the government task force to lockdown the country and in media earlier in the week referenced the Belgian stance.
At the end of September, research emerged on the flaws of the PCR approach in isolation. “When is COVID, COVID?” is a must read for those that are questioning the case dynamic. In summary:
“The PCR test positivity counts should include a standardized threshold level of detection, and at a minimum, the recording of the presence or absence of symptoms. As a disease, the COVID-19 case definition should constitute a disorder that produces a specific set of symptoms and signs. The in-hospital case definition should, therefore, record the CT lung findings and associated blood tests.
Only when an international standard is agreed upon will we be able to make comparisons, and answer the question of when is Covid, Covid?.
Source: https://www.cebm.net/covid-19/when-is-covid-covid/
Time for perspective
There are growing voices in the medical community that we have become too focused on the ‘casedemic’. Some simple statistical facts around well being (rather than a discussion on the economy versus health) that people should reflect on:
- Since June more people have died from pneumonia and seasonal flu in the UK than from COVID (ONS).
- In addition to other severe diseases, mental well being is now a much discussed balancing factor versus COVID (where hospitalisations and deaths have collapsed). Front line medical professionals, in Ireland and Belgium, are seeing significant risks develop. In Ireland, suicide rates in the consumer recession were 30% higher in 2011 versus 2018. Youth unemployment has ramped with the impact on the hospitality and retail sector.
- Outside of high risk groups (elderly and pre-existing conditions) the health risks (resulting in hospitalization and deaths) are in keeping with seasonal flu.
- Medical progress and the antibody discussion is important. As polarising as Trump is at the moment, do not underestimate the significance of the antibody developments in the last week. A cocktail of antibody treatments, like Regeneron and Eli Lilly products, could have a significant impact in the treatment of COVID. Last week, “Emergency Use Authorization” has been sought by the pharma companies to allow access to such treatment outside of a clinical setting. We have spoken to people with knowledge of this area and they do believe in the efficacy of antibody combinations that will help treat genuine cases early and protect the hospital system.
Conclusion
Questions on policy response are growing and people are becoming more balanced about the cure doing more harm than good. Government protocols and media reporting have become very engrained but academics and medical experts are starting to ask questions of the government frameworks. No change of view from the Collective, use this period to be contrarian and acquire shares in leading businesses that will benefit from the post lockdown environment.
The Collective are a panel of stock enthusiasts writing about high conviction investment opportunities with high return potential.
Research
Lot’s more to follow….
Follow us on Twitter or visit our website for more.